Switching to an electric vehicle (EV) has been an exciting step forward, and spending the past 30 days driving the BYD Seal has been a journey of discovery. Covering more than 3,500 km, this experience has reshaped my perspective on EVs, their practicality, and the state of infrastructure in Malaysia.
I purchased the BYD Seal from Macinda EV, a BYD dealer in Kuantan. My sales agent, Ms Kalin, made the process smooth and efficient. She was incredibly nice, knowledgeable, and quick to address any concerns I had. It’s rare to find such outstanding service, and she made the transition to an EV much easier.
A Glimpse into the Future of Driving
What stood out immediately was the BYD Seal’s electronics and smart features. The seamless integration of the car with my phone and wearables has been a revelation. Controlling everything—whether unlocking the car, starting it, or monitoring its stats—feels like stepping into the future. The user-friendly system makes it clear that this is not just a car; it’s a smart device on wheels.
The car itself feels premium, a far cry from outdated stereotypes about Chinese products. BYD has proved that high quality can be affordable. The build is solid, the interior luxurious, and the performance impressive. The torque is exhilarating, and the confidence it gives when overtaking is unmatched. While I have a few complaints (more on that later), the overall package offers excellent value for money.
Planning Every Drive
However, driving an EV in Malaysia is all about planning. With the scarcity of EV chargers, even in a bustling city like Kuala Lumpur, charging requires forethought. Most chargers are still AC, meaning they take a long time to reach a useful level. While the EV landscape is improving, it’s far from ideal for spontaneous long drives.
The multitude of EV charger operators complicates things further. Each has its own app, making it necessary to juggle multiple platforms just to charge your car. This lack of standardisation is frustrating and adds unnecessary hassle. A recent trip highlighted another issue: poor telco coverage delayed my charging session because I couldn’t verify my identity or complete payment. It’s a reminder that EV charging isn’t just about having chargers; the surrounding infrastructure matters just as much.
The Infotainment Could Be Better
One area where BYD could improve is the infotainment system. Built on an Android platform, the interface feels very basic. The fonts, menus, and overall graphics are stock-standard and lack the polish expected from a car of this calibre. It’s an area that feels overlooked in an otherwise premium vehicle.
I’m also not a fan of the rotating screen. While it’s a unique feature, I’d prefer a screen tilted slightly towards the driver for better visibility and ease of use. The rotation adds novelty but doesn’t necessarily enhance functionality, especially when focusing on driving.
The Dashcam Dilemma
One surprising omission in the BYD Seal is the lack of a built-in dashcam. While BYD offers an upgrade to a front-view camera for an additional RM700, I opted to install my own two-channel camera for both the front and back. For those considering a similar route, note that the car’s fuse system uses Micro 2 type fuses, so you’ll need the appropriate tap cable and extra fuses for installation. Alternatively, the BYD camera is a good option if you prefer a sleek, hidden design.
It’s worth noting that newer BYD models, like the Sealion, come with better sensors akin to Tesla’s, improving safety and functionality significantly.
The Technical Details
One aspect that could use improvement is the onboard charger, which is capped at 7 kW. While I’ve opted for a 22 kW wallbox at home, it’s more of an investment for the future than a practical solution today, given the car’s current limitations. For a vehicle as advanced as the BYD Seal, a more robust onboard charger would have been appreciated.
No Going Back
Despite these challenges, driving an EV has been a transformative experience. The smoothness, quietness, and overall driving pleasure are unmatched by internal combustion engine (ICE) vehicles. Once you experience the immediacy and efficiency of an EV, it’s hard to go back. That said, practicality remains a concern, and for now, I still see the need to keep an ICE car as a backup for longer or more unpredictable journeys.
The Verdict
The BYD Seal has delivered far more than I expected, combining premium quality, smart features, and impressive performance at a reasonable price. While Malaysia’s EV infrastructure still has a long way to go, this car proves that EVs are not just the future—they’re the present.
If you’re in Kuantan and considering making the switch to an EV, I highly recommend Ms Kalin at Macinda EV. Her excellent service ensures a hassle-free experience. Additionally, if you’re exploring options, the new BYD Sealion 7 with its impressive 22 kW AC onboard charging capacity, Tesla-like sensors, and better infotainment is a great choice to consider. As the EV ecosystem evolves, the possibilities only grow more exciting.
Recently, I had the privilege of catching up with an old colleague, Professor Razita Sham, who has been appointed as a Professor in the Kulliyyah of Medicine, International Islamic University Malaysia (IIUM). Prof Razita, who is retiring from UNIMAS, and I share a professional history. Although she is more senior than I am, we completed our public health training together at UKM from 1999 to 2003.
Currently, she serves as a short-term consultant for WHO, focusing particularly on One Health. At IIUM, she has been appointed to help with the implementation of the Master of Public Health (MPH) and Doctor of Public Health (DrPH) programmes. Meanwhile, I have been appointed as part of an expert group working on integrating planetary health into higher education, a role I am deeply passionate about.
During our discussion, we delved into the concepts of planetary health and One Health, which seem to be increasingly interconnected in global health discourse. Prof Razita shared an insightful perspective that resonates with me—she sees One Health as a process or approach, and planetary health as the ultimate outcome.
This conceptualisation makes sense. One Health provides a structured, actionable framework. Originating with a focus on food security, it has since expanded to address complex challenges such as zoonosis, where Prof Razita is currently contributing by developing an action plan. One Health’s strength lies in its ability to bring together human, animal, and environmental health experts to address interconnected health issues.
Planetary health, on the other hand, broadens the focus, encompassing the health of the Earth as a system, where human well-being is inextricably tied to the sustainability of natural systems. It represents the ultimate goal—a thriving planet that supports all forms of life, addressing not just zoonotic diseases but also climate change, environmental degradation, and inequities in global health.
While One Health provides clear, actionable steps, planetary health offers a vision of where those actions should lead us. Both are vital in today’s world, where challenges transcend traditional disciplinary boundaries. By integrating these approaches into education and action, we can ensure that the next generation of health professionals and policymakers is prepared to address these global challenges.
My conversation with Prof Razita left me inspired. It reinforced the importance of collaboration, not just across disciplines but also among those working on interconnected frameworks. As we move forward, aligning processes like One Health with outcomes like planetary health is essential for building a healthier, more sustainable future.
It was a pleasant and unexpected meeting, one that reminded me of how far we have come since our training days at UKM, and how much there is still to learn from one another as we navigate the evolving landscape of public and planetary health.
The integration of artificial intelligence (AI) in medicine is transforming healthcare, enabling advanced diagnostics, improved decision-making, and operational efficiencies. However, its application requires careful consideration to ensure that the essence of patient care—ethical responsibility and compassion—is maintained. Clear guidelines are essential to navigate this evolving landscape while simultaneously preparing medical professionals to harness AI effectively through education. As highlighted in a recent article by Hswen and Abbasi (2024), AI lacks emotional intelligence and fiduciary responsibility, which are critical in clinical decision-making. For example, while AI tools can enhance diagnostic accuracy, they cannot “worry” about a patient’s wellbeing or intuitively weigh the moral implications of medical choices.
AI in medicine should always be viewed as a tool to supplement human expertise, not replace it. Tasks requiring moral agency, such as delivering bad news or making ethically complex decisions, must remain the responsibility of clinicians. Transparency is paramount in AI deployment, particularly in patient-facing applications. When patients interact with AI systems, it is ethically imperative that they are informed. Hswen and Abbasi caution against deceptive practices, noting that even unintentional opacity can erode trust. Additionally, the protection of sensitive data must remain a priority. Robust safeguards are needed to prevent unauthorised access or misuse of patient information.
The increasing reliance on AI also sparks the need for a structured framework within medical education. Future clinicians must be equipped to understand, evaluate, and ethically apply AI tools in practice. This involves integrating core competencies such as algorithmic literacy, ethical awareness, and interdisciplinary collaboration into medical curricula. Scenario-based training, where students learn to interpret AI outputs alongside patient care, can provide practical insights. Furthermore, education must emphasise that while AI offers precision and efficiency, compassionate care and human connection remain irreplaceable aspects of medicine.
The future of AI in healthcare extends beyond its current applications. Emerging technologies such as autonomous surgical systems, digital biomarkers, and brain-computer interfaces promise transformative potential. Future research should focus on areas such as personalising care through multi-omics data, integrating AI into lifestyle medicine, and using AI for preventive healthcare. Ethical considerations must guide these advancements. For instance, ensuring that AI systems address, rather than exacerbate, healthcare inequities is crucial. Transparency in algorithm design, patient consent, and cultural sensitivity are essential elements in this process.
AI also holds promise for alleviating administrative burdens, enabling clinicians to dedicate more time to patient interaction. However, as Hswen and Abbasi observe, the unintended consequences of technology—such as increased clinician burnout due to overreliance on electronic systems—must not be overlooked. Efficiency should not come at the cost of quality care or meaningful clinician-patient relationships.
In addition to enhancing clinical practice, AI can revolutionise medical education by enabling adaptive learning and immersive simulations. Generative AI and virtual reality platforms can provide personalised training environments, allowing students to practice high-stakes scenarios. However, these tools must be rigorously tested to ensure alignment with medical evidence and ethical standards. Collaborative research between educators and technologists will be vital to optimise the educational use of AI.
The ethical integration of AI into healthcare requires a multidisciplinary approach, involving clinicians, data scientists, ethicists, and policymakers. As medicine evolves, guidelines and educational frameworks must ensure that technology serves humanity without undermining the moral fabric of care. By balancing innovation with compassion, we can prepare a future where AI enhances healthcare without compromising its core values.
Disclaimer
This article integrates insights from generative AI to enhance its development.
The Central Limit Theorem (CLT) is a fundamental concept in statistics and an essential tool in biostatistics. It provides a foundation for understanding how sample data can be used to make inferences about an entire population. This article will guide students through the development and significance of the CLT, exploring the role of sample means, population means, and the measures of dispersion—particularly the standard error (SE), standard deviation (SD), and confidence interval (CI).
The Origins of the Central Limit Theorem
The CLT emerged in the 18th century through the work of mathematicians like Abraham de Moivre and Pierre-Simon Laplace. De Moivre, while studying probabilities in games of chance, observed that repeated trials formed a bell-shaped distribution. Laplace expanded on this by demonstrating that the sum of independent random variables approximates a normal distribution as the sample size increases. This was a profound realization because it showed that even non-normally distributed data could produce a predictable distribution of means.
Later, Carl Friedrich Gauss solidified the concept of the normal distribution while studying measurement errors in astronomy. Gauss observed that when repeated measurements are taken, the errors typically form a bell-shaped curve. This normal distribution became the foundation for much of statistical analysis, allowing researchers to describe and predict patterns in data.
How the Central Limit Theorem Works
The CLT states that, for a sufficiently large sample size, the distribution of sample means will approximate a normal distribution regardless of the original population’s distribution. This result is powerful because it allows us to use a sample mean as an estimate for the population mean, even when we don’t know the distribution of the underlying data.
In practical terms, the CLT explains why the mean of a sample often provides a reliable estimate of the population mean. As we increase the sample size, the sample mean will tend to get closer to the true population mean, creating the basis for inferential statistics.
Understanding Central Tendency and Dispersion
To make inferences about a population, we need to understand central tendency (mean, median, mode) and dispersion (SD, SE, CI). Central tendency measures provide a summary of where most data points fall, while dispersion measures show how spread out the data points are.
• Mean: The average value of the data points, highly sensitive to outliers.
• Median: The middle value in a sorted dataset, less affected by extreme values.
• Mode: The most frequently occurring value, useful for identifying common outcomes.
In medical research, choosing the correct central tendency measure is important. For instance, in analyzing cholesterol levels among patients, the median might offer a more accurate “central” measure than the mean if the dataset contains extreme outliers.
Measures of Dispersion: SD, SE, and CI
Understanding variability is essential in research, as it indicates how consistent or spread out data points are around the mean. Here’s how SD, SE, and CI are applied:
• Standard Deviation (SD): This measures the spread of data within a sample. A high SD means individual values vary widely around the mean, while a low SD means values cluster closely around the mean.
• Standard Error (SE): This measures how much the sample mean is expected to deviate from the true population mean. The SE decreases as sample size increases, reflecting that larger samples provide more precise estimates of the population mean.
• Confidence Interval (CI): This gives a range within which the population mean likely falls. A 95% CI means we are 95% confident that the interval contains the true population mean. CIs allow researchers to report not only an estimate but also the reliability of that estimate.
Interpreting “Small” SE and CI
What constitutes a “small” SE or CI depends on several factors:
1. Relative Size to the Mean: Typically, an SE or CI that is within 5-10% of the mean can be considered precise in many fields. For example, if the mean blood pressure reduction in a study is 10 mmHg, an SE between 0.5 and 1 mmHg would be considered precise because it reflects only a small percentage (5-10%) of the mean value.
2. Clinical Relevance: In medicine, a small SE or narrow CI must also be clinically meaningful. A small SE that doesn’t offer insight into a meaningful treatment effect wouldn’t necessarily be useful.
3. Sample Size and Precision: SE decreases as sample size increases. Larger samples reduce SE, resulting in narrower CIs, and provide more reliable estimates of the population mean.
Proving Standard Error with R Simulation
To demonstrate that SE accurately represents the precision of the sample mean, we can use a simulation. Here’s an R script that simulates a population, repeatedly samples it, and shows that the simulated SE (standard deviation of sample means) approximates the theoretical SE:
# Set parameters for population population_mean <- 120 # Hypothetical population mean (e.g., blood pressure) population_sd <- 15 # Hypothetical population standard deviation population_size <- 100000 # Large population size for accurate simulation num_samples <- 1000 # Number of samples to draw per sample size
# Generate a large population set.seed(42) population_data <- rnorm(population_size, mean = population_mean, sd = population_sd)
# Define different sample sizes for comparison sample_sizes <- c(10, 50, 100, 500, 1000)
# Create a data frame to store results results <- data.frame(Sample_Size = integer(), Mean_of_Sample_Means = numeric(), Simulated_SE = numeric(), CI_Lower_Bound = numeric(), CI_Upper_Bound = numeric())
# Loop through each sample size and calculate metrics for (sample_size in sample_sizes) { # Draw multiple samples and calculate mean for each sample sample_means <- replicate(num_samples, mean(sample(population_data, sample_size, replace = FALSE)))
# Calculate the mean of sample means, simulated SE, and CI bounds mean_of_sample_means <- mean(sample_means) simulated_se <- sd(sample_means) ci_lower_bound <- mean_of_sample_means - 1.96 * simulated_se ci_upper_bound <- mean_of_sample_means + 1.96 * simulated_se
# Store the results in the data frame results <- results %>% add_row(Sample_Size = sample_size, Mean_of_Sample_Means = mean_of_sample_means, Simulated_SE = simulated_se, CI_Lower_Bound = ci_lower_bound, CI_Upper_Bound = ci_upper_bound) }
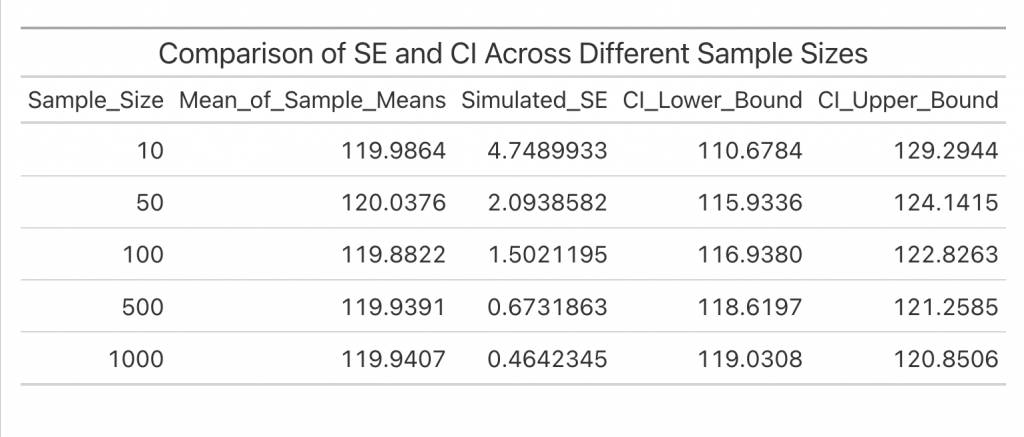
# Display the results table using gt for a neat format results %>% gt() %>% tab_header(title = "Comparison of SE and CI Across Different Sample Sizes")
The output of this simulation with different sample sizes illustrates how SE and CI change with sample size:
Explanation of Results
In this simulation:
• The mean of the sample means should be close to the population mean, confirming that sample means provide a reliable estimate of the true mean.
• The standard deviation of the sample means (simulated SE) will approximate the theoretical SE, supporting that SE reflects how much the sample mean varies from the population mean.
• The decreasing SE and narrowing CI with increasing sample size illustrate that larger samples improve the precision of the sample mean.
Application in Medical Research
In medical research, these measures of dispersion are vital. For instance, in a clinical trial, researchers might measure the mean reduction in blood pressure after a treatment. Reporting the mean reduction alone isn’t enough; they also report SE and CI to show the precision and reliability of this estimate. A smaller SE suggests the sample mean closely approximates the true effect in the population, while the CI gives a range within which the true effect likely falls.
Summary
The Central Limit Theorem and measures like SD, SE, and CI form the statistical backbone of medical research. Through understanding these concepts, researchers can confidently use sample data to estimate population parameters, assess data reliability, and make evidence-based decisions in healthcare.
Disclaimer
This article was created using ChatGPT for educational purposes and should not replace professional statistical advice.
Amid rising global threats from infectious diseases, Malaysia’s Health White Paper (MHW) outlines a national strategy for health security and preparedness, aligning with the WHO’s pathogen prioritisation framework for epidemic and pandemic response. This paper examines the MHW’s focus on pathogen family-based research, surveillance, and international collaboration and assesses its alignment with the WHO’s framework, highlighting key pathogens relevant to Malaysia. Through targeted alignment, Malaysia can enhance its health security infrastructure and capacity to manage emerging and endemic infectious disease threats, thus advancing both national resilience and global health security.
Introduction
The increasing frequency of global infectious disease outbreaks has heightened the urgency for robust national health security frameworks. Malaysia’s Health White Paper (MHW) sets forth a comprehensive strategy, focused on enhancing surveillance, rapid response capabilities, and public health infrastructure to tackle these challenges. The WHO’s pathogen prioritisation framework complements this strategy, advocating for a pathogen family-based approach that emphasises adaptability and international collaboration to fortify preparedness. This paper examines the alignment between Malaysia’s strategic goals and the WHO framework, illustrating how family-based prioritisation, regional contextualisation, and proactive research strengthen Malaysia’s capacity to address significant infectious disease threats.
Pathogen Family-Based Prioritisation and Malaysia’s Health Security Goals
The WHO’s framework prioritises pathogen families, such as Coronaviridae, Flaviviridae, Filoviridae, and Orthomyxoviridae, allowing nations to address a broad range of epidemic threats within high-risk pathogen families (World Health Organization [WHO], 2024). Malaysia’s Health White Paper Pillar 1—Strengthening Health Security—emphasises preparing for both known and emerging threats, including Nipah virus and seasonal influenza. By adopting the WHO’s family-based focus, Malaysia can fortify its capacity for rapid adaptation to pathogens within these families (Ministry of Health Malaysia [MOH], 2024). Priority organisms include SARS-CoV-2 and MERS-CoV (Coronaviridae), Dengue Virus and Zika Virus (Flaviviridae), Ebola Virus (Filoviridae), and various Alphainfluenzavirus strains (Orthomyxoviridae). These pathogens underscore the need for Malaysia to strengthen surveillance and response across related organisms, ensuring preparedness for potential new threats.
Regional Surveillance and Contextualised Research
The WHO framework advocates regional adaptation in surveillance, emphasising pathogen transmission dynamics unique to specific environments and social contexts. This approach is critical in Malaysia, where diseases like dengue, influenced by the tropical climate and high vector presence, pose persistent challenges. Malaysia’s Health White Paper Pillar 2—Strengthening Surveillance and Monitoring—promotes data collection tailored to Malaysia’s specific epidemiology, aligning with WHO’s emphasis on regionalised preparedness (MOH, 2024). Expanding digital health tools and genomic surveillance capabilities will improve Malaysia’s outbreak detection and response, reinforcing the alignment of MHW and WHO goals for region-specific, data-driven preparedness.
Proactive Pathogen Discovery and Prototype Pathogens
To foster proactive pathogen discovery, the WHO framework encourages research on prototype pathogens, supporting the development of medical countermeasures (MCMs) that can apply broadly across pathogen families (WHO, 2024). Pillar 4—R&D and Innovation—of the MHW aligns with this strategy, endorsing investments in health research that facilitate scalable MCM development. By prioritising prototype pathogens like Nipah virus, Malaysia can ensure that advancements in research and countermeasures extend across multiple pathogens within the same family, enhancing resilience against both anticipated and unknown threats.
Closing Knowledge Gaps through Localised Research
Addressing knowledge gaps in transmission, ecology, and host interactions is essential for effective infectious disease management, particularly in Malaysia’s tropical setting, where vector-borne and zoonotic diseases are prominent. The MHW’s Pillar 5—Addressing Health Disparities—emphasises localised public health interventions, bridging critical knowledge gaps in diseases such as leptospirosis and HFMD. This locally focused research aligns with the WHO’s framework, enhancing Malaysia’s capability to develop context-specific interventions based on accurate, regionally relevant data. Prioritising studies on vector ecology, zoonotic interactions, and seasonal transmission dynamics will inform effective policy and public health strategies, meeting both WHO and MHW goals for contextually adapted health responses.
Collaborative Networks for Research and Development
The WHO framework calls for robust international and public-private partnerships to expedite research and preparedness efforts. In the MHW, Pillar 3—Public-Private Partnerships—supports collaborative initiatives within Malaysia’s healthcare ecosystem, facilitating quicker R&D processes and global resource sharing. By engaging in international networks, Malaysia can access critical diagnostic tools, expertise, and resources that align with WHO’s collaborative vision. Establishing networks with regional and global research institutions will enhance Malaysia’s preparedness, supporting WHO’s goals of shared knowledge and resources for infectious disease readiness.
Rapid Deployment of Medical Countermeasures
In line with WHO’s recommendation for rapid MCM deployment, Malaysia’s Health White Paper Pillar 6—Emergency Response Capabilities—prioritises swift resource mobilisation during health crises. Developing MCM stockpiles and streamlined distribution processes will allow Malaysia to respond effectively to pathogens like dengue and influenza, whose rapid spread necessitates immediate intervention. Rapid deployment strategies for critical supplies align with WHO’s framework, advancing Malaysia’s ability to manage high-risk pathogens.
Enhanced Capacity Building and Workforce Development
Effective pathogen preparedness also depends on building healthcare capacity in diagnostics, surveillance, and outbreak management, as emphasised by WHO. The MHW’s Pillar 7—Health Workforce Development—recognises the importance of a well-trained workforce to manage infectious disease threats. By equipping healthcare professionals with skills in diagnostics, genomic analysis, and rapid response, Malaysia supports WHO’s vision of strengthening national capacity for public health resilience. Expanding training programs and building diagnostic expertise will enable Malaysia to maintain an agile and effective response to public health threats, enhancing preparedness at both local and global levels.
Conclusion
The alignment between Malaysia’s Health White Paper and the WHO’s pathogen prioritisation framework establishes a comprehensive foundation for infectious disease preparedness. By incorporating the WHO’s recommendations for pathogen family prioritisation, regional surveillance, and collaborative partnerships, Malaysia’s health system is well-positioned to tackle both current and emerging infectious disease challenges. Through targeted initiatives in surveillance, research, and rapid response, Malaysia strengthens its role in global health security while enhancing national resilience to future public health emergencies.
Disclaimer: This paper includes insights generated by ChatGPT and should be reviewed and validated by experts before any formal use.
References
Ministry of Health Malaysia. (2024). Malaysia Health White Paper: Strategic Directions in Health Security.
World Health Organization. (2024). Pathogen prioritization framework for epidemic and pandemic preparedness. WHO.
Imagine that every swan observed in a particular region is white, leading to the belief that “all swans are white.” This conclusion appears reliable until the unexpected discovery of a black swan, which disproves this assumption. This example demonstrates a fundamental principle of hypothesis testing: science is often less about proving ideas to be universally true and more about disproving them to allow for further understanding. The discovery of a black swan challenges the certainty of the prior belief and highlights the scientific value of testing and questioning.
A similar principle operates in the legal system, particularly in criminal trials. Here, the defendant is presumed “not guilty” until proven otherwise. This presumption of innocence serves as a null hypothesis, establishing a baseline assumption that remains in place unless substantial evidence refutes it. The burden of proof lies with the prosecution to present sufficient evidence to reject the “not guilty” assumption. If the evidence does not meet the required threshold, the verdict is “not guilty.” However, a verdict of “not guilty” does not equate to proof of innocence; it merely indicates that there was not enough evidence to reject the initial assumption. This cautious approach minimises errors in the justice process, underscoring the importance of evidence-based decision-making.
In scientific research, hypothesis testing operates on a similar foundation, using a “null hypothesis” that provides a default assumption, usually stating that there is no effect or difference. Statisticians like Ronald A. Fisher developed hypothesis testing methods to structure scientific inquiry. Researchers gather data to test whether there is enough evidence to reject the null hypothesis. This method ensures that claims are only accepted when supported by statistically significant evidence, reducing the chance of errors.
Why Rejection is Easier than Acceptance
It is easier to prove that not all swans are white than to prove that every swan is white, as a single black swan is enough to challenge this certainty. In hypothesis testing, we often start with a “no effect” or “no difference” assumption because it allows us to look for evidence that disproves it rather than trying to prove a universal truth.
Imagine researchers are testing a new drug intended to improve cancer survival rates compared to the standard treatment.
• Null Hypothesis (H₀): The new drug does not improve survival rates compared to the standard treatment (no effect).
• Alternative Hypothesis (H₁): The new drug does improve survival rates compared to the standard treatment.
Here, the null hypothesis assumes no improvement with the new drug. By starting with this “no effect” assumption, researchers have a neutral basis for testing. If there’s strong evidence against the null hypothesis, they can reject it in favour of the alternative.
Researchers conduct a trial with two groups of patients: one receiving the new drug and the other receiving the standard treatment. If they observe significantly higher survival rates in the group taking the new drug, they calculate the probability of seeing this difference under the assumption of “no effect.” If the probability of achieving these results by chance alone is very low (for example, below 5%, or p-value < 0.05), it suggests that the survival benefit observed is unlikely if the drug truly had no effect. This gives researchers grounds to reject the null hypothesis and conclude that the drug likely improves survival rates.
To reject the null hypothesis, researchers only need a few trials showing significant improvement with the new drug to question the “no effect” assumption. But to prove that the drug universally improves survival rates in every case would require countless trials and still wouldn’t provide absolute certainty.
Beyond Detecting Differences
In hypothesis testing, the traditional approach often aims to detect a difference between groups or treatments, such as whether a new drug performs better than an existing one. However, researchers sometimes have different objectives, and other types of hypotheses can better reflect these specific goals. These include superiority, non-inferiority, and equivalence hypotheses, each of which frames the research question in a distinct way.
Superiority Hypothesis: This hypothesis seeks to determine whether one treatment is better than another. For example, testing whether a new cancer drug improves survival rates more than the current standard drug. Here, the null hypothesis assumes the new treatment is no better than the standard, while the alternative suggests the new treatment is superior. If the data shows a statistically significant improvement with the new treatment, researchers can reject the null hypothesis and conclude that the new drug is likely superior.
Non-Inferiority Hypothesis: In some studies, the goal is to show that a new treatment is not worse than the existing standard by more than an acceptable margin. This is often used when the new treatment may have other benefits, such as being less costly or easier to administer. For instance, researchers might test whether a new oral medication for high blood pressure is not significantly less effective than an injectable option, but is easier to use. Here, the null hypothesis assumes that the new treatment is worse than the standard by more than the acceptable margin, while the alternative hypothesis is that it is not worse. Results within the non-inferiority margin allow researchers to reject the null hypothesis and conclude that the new treatment is non-inferior.
Equivalence Hypothesis: This hypothesis tests whether two treatments produce similar effects within a specified range. Equivalence studies are useful when researchers want to show that a new treatment performs just as well as an existing one, typically to confirm that the new treatment can replace the current standard without loss of efficacy. For example, researchers might test whether a generic drug is as effective as a brand-name drug within a small acceptable range of difference. The null hypothesis here assumes the treatments differ by more than the acceptable range, while the alternative suggests they are equivalent. Rejecting the null hypothesis indicates that the treatments can be considered interchangeable.
Errors in Hypothesis Testing
Hypothesis testing involves managing the risks of two main errors:
Type I Error (False Positive): This error occurs when a true null hypothesis is incorrectly rejected. In a medical context, this could mean diagnosing a patient with a disease they do not actually have. Such an error could lead to unnecessary anxiety, additional tests, or even unnecessary treatment. In statistical terms, the probability of a Type I error is represented by alpha (α), usually known as the p-value, and is often set at 0.05.
In hypothesis testing, the p-value helps us determine whether the results we observe are likely to reflect the real truth—an actual effect of the treatment—or are simply due to chance. When we talk about the “truth” in this context, we’re asking if the observed benefit of a new drug (for instance, an improvement in cancer survival rates) is genuinely due to the drug itself, rather than a random occurrence. The goal of statistical testing is to help us differentiate between results that reflect real-world effects and those that could have happened by coincidence.
Type II Error (False Negative): This error occurs when a false null hypothesis is not rejected. In medical testing, this would be failing to diagnose a patient who actually has the disease, potentially leading to missed treatment. The probability of a Type II error is represented by beta (β), with the power of a test (1 – β) reflecting its ability to detect true effects.
Both errors have real-world implications, especially in medicine, where incorrectly diagnosing a healthy patient (Type I error) or missing a diagnosis in an ill patient (Type II error) can have significant consequences.
Looking Beyond Numbers
The white swan story, the legal system, and hypothesis testing share a common theme: reliable conclusions require rigorous evidence and careful judgment. Hypothesis testing isn’t only about calculating probabilities and p-values; it’s about interpreting what those numbers mean in real-world contexts. By prioritising the rejection of assumptions rather than their acceptance, science follows a cautious, methodical path that allows for meaningful and reliable discoveries. This approach encourages researchers to look beyond statistical outcomes alone and consider the larger implications of their findings. Through thorough testing and the careful interpretation of evidence, hypothesis testing fosters a structured and reliable process for understanding the world.
In the modern landscape of education and community engagement, success has long been measured by outputs—metrics like the number of publications, course completions, or participants reached. While these indicators of process are essential, they often offer only a superficial view of the real-world change that such efforts can achieve. True impact extends beyond these processes, reaching deeper levels of personal and societal transformation. Impact affects various spheres: individuals who experience personal growth, families whose values and dynamics are enriched, communities that gain cohesion, institutions that drive meaningful progress, nations that grow in stability and well-being, and even the planet, which benefits from sustainable practices and global cooperation. By shifting our focus from process to impact, we can foster change that is both meaningful and lasting.
Understanding Impact
Impact in education and community work can be conceptualised as the tangible, enduring benefits that result from these initiatives, spanning multiple levels. At the personal level, education or community engagement fosters individual growth, strengthening personal values and building resilience (Bryson et al., 2020). This transformation often extends to family dynamics, where these newly acquired values shape interactions, fostering environments that support learning, empathy, and well-being (World Health Organization [WHO], 2017). At the community level, the process of engagement is critical; however, true impact occurs when communities transform in ways that reflect growth and shared values, addressing issues from literacy to healthcare access (Fraser et al., 2019). Institutional impact further amplifies this by driving policies, shaping curricula, and creating initiatives that reinforce societal values and equity. Nationally, impactful education produces skilled professionals and engaged citizens, contributing to financial stability, political resilience, and sustainable progress (UNESCO, 2015). Ultimately, the ripple effect of these transformations has the potential to address global challenges, fostering planetary health and sustainability (Crawford et al., 2021).
Why Impact Matters
Aligning Actions with Purpose
While output-based metrics track the processes of learning, such as course completion rates or publication counts, focusing on impact reorients efforts toward purpose. This approach ensures that educational and research activities are truly meaningful, working to create compassionate professionals, sustainable communities, or informed citizens. In medical education, for example, impact could be measured by improved patient outcomes rather than just the number of doctors trained (Bryson et al., 2020).
Creating Sustainable Change
A focus on impact cultivates changes that endure beyond the lifespan of a project. In community health, for example, a programme aimed at reducing disease prevalence may have sustainable impact if it results in long-term behavioural change, such as improved hygiene practices or healthier lifestyle choices among community members (Green et al., 2018). Sustainable transformation, as opposed to temporary gains, requires that the underlying values and practices endure over time, leading to lasting benefits for individuals and societies.
Encouraging Accountability
Evaluating impact holds educators, researchers, and community leaders accountable not only for the processes they initiate but also for the long-term effects of their work. Questions of impact shift the focus from quantitative outputs to qualitative change, asking whether a project has improved social values, supported financial sustainability, or contributed to political stability (UNESCO, 2015). This accountability framework enhances the integrity of educational and research programmes by ensuring they deliver genuine societal benefits.
Enhancing Financial and Social Value
Focusing on impact also supports the wise allocation of resources, with funding directed towards projects that yield significant, long-term benefits. Financial impact can be seen in economic resilience, as educational programmes improve employability and health initiatives reduce public healthcare costs (Crawford et al., 2021). Social value is equally crucial; by promoting equity, inclusion, and community welfare, impactful initiatives strengthen the social fabric and build resilience.
Addressing Global Challenges and Planetary Health
Educational and research institutions, by aligning with the United Nations Sustainable Development Goals (SDGs), can actively contribute to planetary health and sustainability (UNESCO, 2015). For instance, research that advances environmental literacy or fosters sustainable practices directly supports global sustainability goals, emphasising that every local initiative has the potential to contribute to a healthier planet.
Measuring Impact Beyond Traditional Metrics
Impact measurement requires a nuanced approach, utilising tools and methods that capture both immediate and long-term effects across multiple domains. Personal growth can be assessed through reflective evaluations and surveys that track changes in values and behaviours (WHO, 2017). Community impact might involve participatory research methods that gather qualitative insights from community members, while financial sustainability can be gauged through Social Return on Investment (SROI) analyses, which quantify economic benefits against costs (Green et al., 2018). Policy analysis can measure political impact, tracing how research influences governance or legislative change (Bodilly et al., 2017). At the planetary level, environmental impact assessments aligned with SDG metrics allow institutions to measure contributions toward global sustainability (Crawford et al., 2021).
The Role of University Rankings in Measuring Impact
Increasingly, university ranking systems are recognising the importance of impact-focused metrics, moving beyond traditional outputs to capture the broader contributions of institutions to society and the environment. The Times Higher Education (THE) Impact Rankings evaluates universities based on their alignment with the United Nations Sustainable Development Goals (SDGs), offering insights into how institutions address global challenges such as poverty and health (Times Higher Education, n.d.). The QS Stars University Rating System includes an “Impact” category that assesses community engagement and social responsibility (QS Quacquarelli Symonds, n.d.), while the UI GreenMetric World University Rankings specifically measures environmental sustainability practices on campuses (Universitas Indonesia, 2023). U-Multirank, funded by the European Commission, takes a multidimensional approach that includes regional engagement and knowledge transfer, allowing for a more nuanced assessment of local impact (U-Multirank, n.d.). These rankings encourage universities to prioritise sustainable practices, community engagement, and social responsibility, fostering a global movement towards impact-driven education.
A Future Built on Impact
As we navigate the future of education, research, and community engagement, a focus on impact is essential for creating meaningful, lasting change. This approach reframes educational initiatives as investments in personal development, family and social values, financial resilience, political stability, and planetary health. By integrating these dimensions into the core of educational and research efforts, institutions can drive progress on multiple fronts, fostering a more resilient, equitable, and sustainable society. In essence, a shift from process to impact enables us to fulfil not only the immediate goals of education and research but also the broader, transformative changes that these fields can inspire.
Disclaimer: This article was created using OpenAI’s ChatGPT for research and educational purposes.
References
Bodilly, S. J., Chun, J., Ikemoto, G. S., & Stockly, S. (2017). Improving school leadership: The promise of cohesive leadership systems. Rand Corporation.
Bryson, J. M., Patton, M. Q., & Bowman, R. A. (2020). Working across boundaries: Making collaboration work in government and nonprofit organizations. John Wiley & Sons.
Crawford, M., Hoque, Z., & Moll, J. (2021). Public sector reform and performance management: Managing on the edge. Routledge.
Fraser, N., Bunting, M., & O’Brien, M. (2019). Community engagement: Key to better health and education outcomes. World Health Organization.
Green, C., Hinton, P., & Ridley, M. (2018). Sustainable health and community development: Building resilience and equity. Oxford University Press.
Times Higher Education. (n.d.). Impact Rankings 2023. Times Higher Education. https://www.timeshighereducation.com/impactrankings
U-Multirank. (n.d.). What is U-Multirank? https://www.umultirank.org
UNESCO. (2015). Education 2030: Incheon declaration and framework for action towards inclusive and equitable quality education and lifelong learning for all. UNESCO.
Universitas Indonesia. (2023). UI GreenMetric World University Rankings 2023. Universitas Indonesia. https://greenmetric.ui.ac.id/
World Health Organization. (2017). Community engagement framework for quality, people-centered, and resilient health services. WHO.
The evolving demands on healthcare systems worldwide have highlighted the need for direct-care physicians to adopt educational roles. A recent JAMA article by Sweigart, Watson, and Burger (2024) emphasises this trend, explaining that more physicians are being called upon to act as educators as training expands to new healthcare settings. This development is particularly relevant in Malaysia, where the demand for medical specialists continues to rise and where expanding training locations can address both capacity challenges and geographic disparities in specialist availability.
Malaysia’s medical specialist training is currently provided primarily by local universities, including both public and private institutions. These university-based programmes, while well-established, face limitations in the number of trainees they can accommodate. With the need for specialists projected to grow significantly, Malaysia must look beyond universities to scale up training opportunities. Increasing the number of Ministry of Health (MOH) hospitals involved in training offers a promising solution. By incorporating more MOH hospitals, especially in Sabah and Sarawak, Malaysia can provide specialist training opportunities close to home for doctors in these regions, reducing the need for them to relocate to Peninsular Malaysia. This decentralised approach aligns with the Ministry of Health’s objectives to improve healthcare accessibility across the country and to support equitable healthcare distribution.
Expanding training locations, however, brings forth the critical need to maintain quality and consistency across all settings. To ensure that trainees receive a high-quality, uniform education, a standardised curriculum is essential. The National Postgraduate Medical Curriculum (NPMC), developed by the Malaysian Public University Medical Deans Council under the Ministry of Higher Education, plays a pivotal role in addressing this need. The NPMC provides structured learning objectives, competency benchmarks, and assessment methods, ensuring that all trainees, regardless of training location, are prepared to meet the same rigorous standards. This curriculum, authored by experts nationwide, is designed to ensure that the training of specialists in Malaysia aligns with the country’s healthcare needs and meets the standards expected in modern medical practice (Amjad, 2024).
For this initiative to succeed, collaboration between universities and the Ministry of Health is essential. Universities bring established expertise in medical education, while MOH hospitals provide diverse clinical settings and cases essential for comprehensive training. A coordinated effort between these institutions can bridge the gap between academia and practical, patient-focused training. This collaboration can involve sharing resources, co-developing faculty development programmes to prepare MOH clinicians for teaching roles, and creating mentorship opportunities to support trainee learning in non-university settings. This integrated approach, as outlined in the JAMA article, requires that both universities and hospitals embrace the dual responsibilities of patient care and education to develop a future-ready healthcare workforce (Sweigart et al., 2024).
Through the combined efforts of universities, the MOH, and other stakeholders, Malaysia has an opportunity to create a sustainable and resilient specialist training framework. By expanding training locations to MOH hospitals, particularly in underrepresented regions, and implementing the NPMC, Malaysia can ensure that future specialists receive consistent, high-quality education across diverse settings. This strategy not only addresses the immediate need for increased specialist training capacity but also supports the broader goal of equitable healthcare distribution throughout the country.
Disclaimer: This article was generated with assistance from ChatGPT, an AI language model.
References
Amjad, N. M. (2024). Postgraduate clinical specialist training in Malaysia: At a crossroads. International Medical Journal Malaysia, 23(2), 1–3. Retrieved from https://journals.iium.edu.my/kom/index.php/imjm/article/download/2583/1483/16082
Sweigart, J. R., Watson, R., & Burger, A. (2024). The accidental teacher—Direct-care physicians increasingly placed in teaching roles. JAMA. https://doi.org/10.1001/jama.2024.17626
Reluctant I stood, thrust into this place, Not chosen by will, yet I embrace the grace, A weight I carry, solemn and true, Guided by purpose, though unsure of the view.
Time fades to whispers, deadlines blur, I heed no pressure from titles that stir, If power deems me fit to leave, Indifference shields what I believe.
Climbing the curve, each step uphill, Learning the dreams this place fulfills, A vision uncovered, first small, then wide, A call to the country, seen from inside.
Through my eyes, it grew, a daunting sight, To share with others, to bridge the light, Struggling to bring all minds as one, The task never finished, yet hardly begun.
Alone in thought, as shadows fall, Wrestling with doubts that stand so tall, A quiet fear this role has changed What once felt certain, now feels strange.
So I ask for guidance, Allah above, To keep my soul, to lead with love, May wisdom hold what pride may sway, And mercy light my lonely way.
The MBBS programme is designed to produce doctors who are competent, compassionate, and safe. This aim extends beyond technical proficiency to cultivate healthcare professionals who are ethically driven, empathetic, and dedicated to the wellbeing of both their patients and society at large. As the world faces increasingly complex health challenges due to environmental crises, these qualities of compassion and competency must also extend to planetary health. Recognising the profound connections between human and environmental health, doctors today must be prepared to understand and address health issues within a broader ecological context.
Moreover, the future of healthcare is uncertain, and doctors will confront unknown and unpredictable challenges. Emerging diseases, environmental degradation, and new public health threats will require healthcare professionals who are adaptable, forward-thinking, and equipped to approach health holistically. Integrating planetary health into the MBBS curriculum aligns with these objectives, preparing future doctors to respond to the interwoven challenges of environmental and human health. Through the framework of Education for Sustainable Development (ESD) and recent updates to the Malaysian Qualifications Framework (MQF), medical educators can seamlessly incorporate planetary health principles without increasing total learning time. This paper outlines how these concepts can be embedded within the existing curriculum, equipping the next generation of doctors to safeguard both human health and environmental sustainability in an unpredictable future.
Understanding Planetary Health, Sustainability, OneHealth, and Nature-Based Solutions
Planetary health, sustainability (specifically, the Sustainable Development Goals or SDGs), OneHealth, and nature-based solutions (NbS) are interconnected yet distinct approaches within environmental and health frameworks. Here’s a comparison:
Focuses on how environmental health affects human wellbeing (Whitmee et al., 2015; Myers & Frumkin, 2020)
Specifically targets interactions between human, animal, and environmental health, particularly zoonotic diseases (Rabinowitz et al., 2018)
Practical actions that protect, sustainably manage, or restore ecosystems to address societal and health challenges (IUCN, 2023)
Primary Goal
To balance current needs with preserving resources and stability for future generations (United Nations, 2015)
To protect human health by safeguarding natural ecosystems and addressing environmental risks (Whitmee et al., 2015)
To address health risks at the intersection of human, animal, and environmental health, especially focusing on zoonoses
To leverage natural systems to enhance resilience and provide ecosystem services that benefit both human and planetary health (IUCN, 2023)
Focus Areas
Resource management, waste reduction, social equity, economic stability, and environmental protection (Raworth, 2017)
Human health impacts from climate change, pollution, and ecosystem degradation (Prescott & Logan, 2019; Myers & Frumkin, 2020)
Zoonotic disease control, ecosystem health, and the interconnectedness of human and animal health (Rabinowitz et al., 2018)
Climate change adaptation, ecosystem restoration, green infrastructure, urban green spaces, and sustainable agriculture (World Economic Forum, 2024)
Applications
Multisectoral approach: energy, agriculture, economics, social policy, etc. (United Nations, 2015)
Primarily within healthcare and public health, with a focus on preventing environmental impacts on human health (Myers & Frumkin, 2020)
Predominantly used in infectious disease control, veterinary science, and environmental health
Used in urban planning, public health, climate resilience, water management, and more (IUCN, 2023; World Economic Forum, 2024)
Relationship to Health
Indirect: Sustainable practices support health by maintaining stable resources and healthy environments (Raworth, 2017)
Direct: Addresses how environmental degradation leads to immediate and long-term health impacts on populations
Direct: Examines the specific health implications of human-animal-environment interactions, focusing on shared diseases
Direct: NbS provide ecosystem services that enhance air and water quality, reduce disease vectors, and promote mental and physical wellbeing (IUCN, 2023)
Scope Comparison
Broader scope, incorporating planetary health as a subset (United Nations, 2015)
More focused within sustainability, specifically relating to environmental impacts on health (Whitmee et al., 2015)
Narrowest scope, focusing specifically on health issues arising from human-animal-environment interactions (Rabinowitz et al., 2018)
Targeted approach within planetary health, using ecosystems to deliver sustainable health and environmental outcomes (World Economic Forum, 2024)
This table clarifies that sustainability is the broadest framework, with planetary health focusing on environmental impacts on human wellbeing. OneHealth and NbS are more specific, with NbS providing actionable solutions that align with both planetary and human health.
The Role of Nature-Based Solutions in Planetary Health and Medical Education
Nature-based solutions, supported by frameworks like those from the International Union for Conservation of Nature (IUCN), are integral to planetary health, providing ecosystem services that benefit human wellbeing. Examples include the role of green urban spaces in reducing respiratory diseases, wetlands in water purification, and mangroves in coastal resilience. Pharmaceutical companies are also beginning to invest in NbS, recognising their importance in sourcing medicinal compounds sustainably and supporting biodiversity that mitigates disease spread (World Economic Forum, 2024).
By incorporating NbS concepts into medical education, future healthcare professionals can better understand how ecosystem health directly impacts human health. This approach allows doctors to recommend preventive strategies that support both individual and community health, aligning with planetary health goals.
Seamless Integration of Planetary Health and NbS in Medical Education
Nature-based solutions can be seamlessly integrated into MBBS modules. Here’s a structure for how these topics align with existing curriculum goals:
1. Physiology and Pathology
• Embed environmental factors, such as pollution and climate change, in discussions of respiratory and cardiovascular health.
• Include studies on nanoplastic exposure and its potential inflammatory effects in cardiovascular health modules (Jin et al., 2022).
• Integrate the effects of urban green spaces on lowering rates of respiratory diseases due to reduced pollution and increased physical activity.
2. Community Medicine and Public Health
• Teach how NbS can mitigate vector-borne diseases, such as dengue and malaria, by restoring wetlands and promoting urban green spaces.
• Discuss the importance of sustainable food systems within nutrition topics, linking agroforestry practices with improved nutrition and reduced pesticide use (World Economic Forum, 2024).
• Explore mental health benefits of nature exposure, using urban green space initiatives as a case study.
3. Pharmacology
• Examine sustainable medicinal sourcing and the role of biodiversity in providing plant-based medicines. Pharmaceutical companies’ investments in biodiversity protection reflect this approach (World Economic Forum, 2024).
• Discuss antibiotic stewardship to prevent environmental contamination and antimicrobial resistance (Singer et al., 2019).
4. Clinical Rotations
• Include case studies that address health impacts of environmental changes, such as heat-related illnesses and waterborne diseases from pollution and ecosystem degradation.
• Emphasize NbS as community-level solutions in clinical practice, such as recommending exposure to green spaces for stress management and discussing community advocacy for clean water and air.
Expected Outcomes of Integrating Planetary Health and NbS
Aligned with the updated MQF and ESD principles, the following are the expected outcomes for medical graduates 4-5 years after completing a curriculum that integrates planetary health and NbS:
1. Holistic Patient Care with Planetary Health Awareness
Graduates will deliver patient care that considers environmental factors affecting health, advising patients on lifestyle choices that support both personal and planetary wellbeing.
2. Advocacy for Sustainable Healthcare
Graduates will promote sustainable practices in healthcare settings, such as reducing waste, supporting biodiversity, and conserving energy, contributing to planetary health goals.
3. Community Engagement and Environmental Health Advocacy
Graduates will educate communities on the benefits of NbS, advocating for policies that promote health through clean air, water, and urban greenery.
4. Ethical Responsibility in Environmental Health
Graduates will understand their role in promoting ecosystem protection as a foundation for health, supporting efforts to reduce health disparities related to environmental degradation.
Recommendations
Integrating planetary health and NbS into the MBBS curriculum, without adding new topics, enriches medical education by promoting a global awareness of health interdependencies. This integration equips doctors to address health in ways that support human and environmental sustainability, making a positive impact on society and the planet.
Disclaimer
This article was created with assistance from ChatGPT, an AI language model, to provide an overview of integrating planetary health into medical education. While the content has been reviewed to ensure accuracy and relevance, readers are encouraged to consult additional sources and expert opinions when implementing educational frameworks.
References
International Union for Conservation of Nature. (2023). Nature-based solutions. Retrieved from https://iucn.org/our-work/nature-based-solutions
Jin, H., Ma, T., Sha, X., Liu, Z., & Zhou, Y. (2022). Nanoplastics and cardiovascular diseases: A link from the environment to human health. Environmental Research, 204, 112281. https://doi.org/10.1016/j.envres.2021.112281
Landrigan, P. J., Fuller, R., Acosta, N. J. R., Adeyi, O., Arnold, R., Basu, N., & Zhong, M. (2018). The Lancet Commission on pollution and health. The Lancet Planetary Health, 2(1), e26-e36. https://doi.org/10.1016/S2542-5196(17)30173-8
Lim, S. S., Vos, T., Flaxman, A. D., Danaei, G., Shibuya, K., Adair-Rohani, H., & Ezzati, M. (2021). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2224-2260. https://doi.org/10.1016/S0140-6736(12)61766-8
Myers, S. S., & Frumkin, H. (2020). Planetary health: Protecting nature to protect ourselves. Island Press.
Prescott, S. L., & Logan, A. C. (2019). Planetary health: From the wellspring of holistic medicine to personal and public health imperative. Explore, 15(2), 98-106. https://doi.org/10.1016/j.explore.2018.11.008
Prüst, M., Meijer, J., Westerink, R. H., & Brouwer, A. (2020). The plastic brain: Neurotoxicity of micro- and nanoplastics. Environmental Science & Technology, 54(18), 11431-11441. https://doi.org/10.1021/acs.est.0c02350
Rabinowitz, P. M., Natterson-Horowitz, B., Kahn, L. H., & Kock, R. (2018). One Health and Planetary Health: Perspectives from the U.S. National Institutes of Health. National Institutes of Health.
Raworth, K. (2017). Doughnut economics: Seven ways to think like a 21st-century economist. Chelsea Green Publishing.
Singer, A. C., Shaw, H., Rhodes, V., & Hart, A. (2019). Review of antimicrobial resistance in the environment and its relevance to environmental management in the context of planetary health. The Lancet Planetary Health, 3(7), e253-e261. https://doi.org/10.1016/S2542-5196(19)30078-1
United Nations. (2015). Transforming our world: The 2030 Agenda for Sustainable Development. Sustainable Development Goals (SDGs). Retrieved from https://sdgs.un.org/2030agenda
Whitmee, S., Haines, A., Beyrer, C., Boltz, F., Capon, A. G., Dias, B. F., & Yach, D. (2015). Safeguarding human health in the Anthropocene epoch: Report of The Rockefeller Foundation–Lancet Commission on planetary health. The Lancet, 386(10007), 1973-2028. https://doi.org/10.1016/S0140-6736(15)60901-1
World Economic Forum. (2024). How pharma companies are investing in nature to improve human and planetary health. Retrieved from https://www.weforum.org/stories/2024/09/how-pharma-companies-are-investing-in-nature-to-improve-human-and-planetary-health/